Addressing the Challenge of Hidden Hunger
The ‘hidden hunger’ due to micronutrient deficiency does not produce hunger as we know it. You might not feel it in the belly, but it strikes at the core of your health and vitality.
- Kul C. Gautam, former deputy executive director of UNICEF
Note: The views expressed in this chapter are those of the author. They do not necessarily reflect the views of IFPRI, Welthungerhilfe, or Concern Worldwide.
Box 3.1
DEFINITIONS
-
Hunger: distress related to lack of food
-
Malnutrition: an abnormal physiological condition, typically due to eating the wrong amount and/or kinds of foods; encompasses undernutrition and overnutrition
-
Undernutrition: deficiencies in energy, protein, and/or micronutrients
-
Micronutrient deficiency (also known as hidden hunger): a form of undernutrition that occurs when intake or absorption of vitamins and minerals is too low to sustain good health and development in children and normal physical and mental function in adults. Causes include poor diet, disease, or increased micronutrient needs not met during pregnancy and lactation
-
Undernourishment: chronic calorie deficiency, with consumption of less than 1,800 kilocalories a day, the minimum most people need to live a healthy, productive life
-
Overnutrition: excess intake of energy or micronutrients
Sources: FAO (2013); and von Grebmer et al. (2013).
Hidden hunger, also known as micronutrient deficiencies, afflicts more than 2 billion individuals, or one in three people, globally (FAO 2013). Its effects can be devastating, leading to mental impairment, poor health, low productivity, and even death. Its adverse effects on child health and survival are particularly acute, especially within the first 1,000 days of a child’s life, from conception to the age of two, resulting in serious physical and cognitive consequences.
Even mild to moderate deficiencies can affect a person’s well-being and development. In addition to affecting human health, hidden hunger can curtail socioeconomic development, particularly in low and middle income countries.
A Different Kind of Hunger
Hidden hunger is a form of undernutrition that occurs when intake and absorption of vitamins and minerals (such as zinc, iodine, and iron) are too low to sustain good health and development (Box 3.1).
Factors that contribute to micronutrient deficiencies include poor diet, increased micronutrient needs during certain life stages, such as pregnancy and lactation, and health problems such as diseases, infections, or parasites.
While clinical signs of hidden hunger, such as night blindness due to vitamin A deficiency and goiter from inadequate iodine intake, become visible once deficiencies become severe, the health and development of a much larger share of the population is affected by less obvious “invisible” effects. That is why micronutrient deficiencies are often referred to as hidden hunger.
The Global Hidden Hunger Crisis
 Source: Black et al. (2013).
Source: Black et al. (2013).
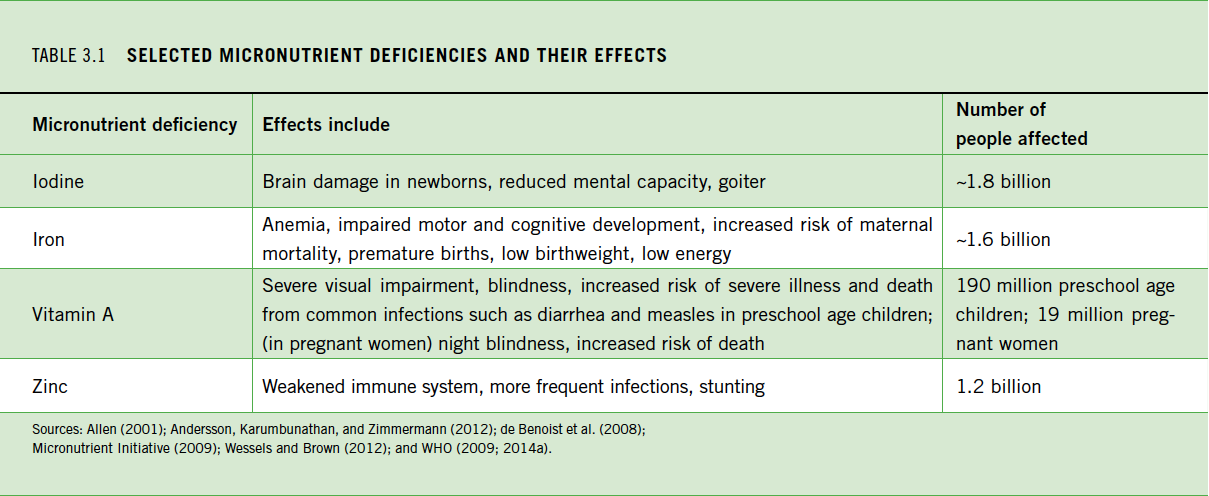 Sources: Allen (2001); Andersson, Karumbunathan, and Zimmermann (2012); de Benoist et al. (2008); Micronutrient Initiative (2009); Wessels and Brown (2012); and WHO (2009; 2014a).
Sources: Allen (2001); Andersson, Karumbunathan, and Zimmermann (2012); de Benoist et al. (2008); Micronutrient Initiative (2009); Wessels and Brown (2012); and WHO (2009; 2014a).
 Source: Adapted from ACC/SCN (2000).
Source: Adapted from ACC/SCN (2000).
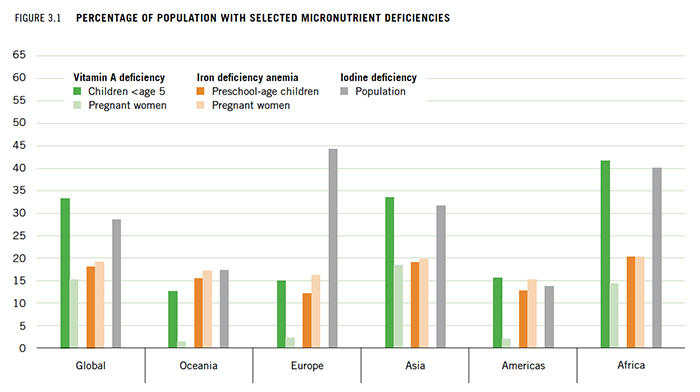
More than 2 billion people worldwide suffer from hidden hunger, more than double the 805 million people who do not have enough calories to eat (FAO, IFAD, and WFP 2014). Much of Africa south of the Sahara and the South Asian subcontinent are hotspots where the prevalence of hidden hunger is high (Figure 3.1 [right]). The rates are relatively low in Latin America and the Caribbean where diets rely less on single staples and are more affected by widespread deployment of micronutrient interventions, nutrition education, and basic health services (Weisstaub and Araya 2008). Although a larger proportion of the burden of hidden hunger is found in the developing world, micronutrient deficiency, particularly iron and iodine deficiency, is also widespread in the developed world (Figures 3.1 [right] and 3.2 [below]).
The nature of the malnutrition burden facing the world is increasingly complex. Developing countries are moving from traditional diets based on minimally processed foods to highly processed, energy-dense, micronutrient-poor foods and drinks, which lead to obesity and diet-related chronic diseases. With this nutrition transition, many developing countries face a phenomenon known as the “triple burden” of malnutrition—undernourishment, micronutrient deficiencies, and obesity (Pinstrup-Andersen 2007). In higher income, more urbanized countries, hidden hunger can coexist with overweight/obesity when a person consumes too much dietary energy from macronutrients such as fats and carbohydrates (Guralnik et al. 2004). While it may seem paradoxical, an obese child can suffer from hidden hunger.
Micronutrient deficiencies cause an estimated 1.1 million of the 3.1 million child deaths that occur each year as a result of undernutrition (Black et al. 2013; Black et al. 2008). Vitamin A and zinc deficiencies adversely affect child health and survival by weakening the immune system. Lack of zinc impairs growth and can lead to stunting in children. Iodine and iron deficits prevent children from reaching their physical and intellectual potential (Allen 2001).
Women and children have greater needs for micronutrients (Darnton-Hill et al. 2005). The nutritional status of women around the time of conception and during pregnancy has long-term effects for fetal growth and development. Nearly 18 million babies are born with brain damage due to iodine deficiency each year. Severe anemia contributes to the death of 50,000 women in childbirth each year. In addition, iron deficiency saps the energy of 40 percent of women in the developing world (UNSCN 2005; Micronutrient Initiative 2014). Interventions to fight hidden hunger and improve nutrition outcomes generally focus on women, infants, and young children. By targeting these populations, interventions achieve high rates of return by improving health, nutritional status, and cognition later in life (Hoddinott et al. 2013).
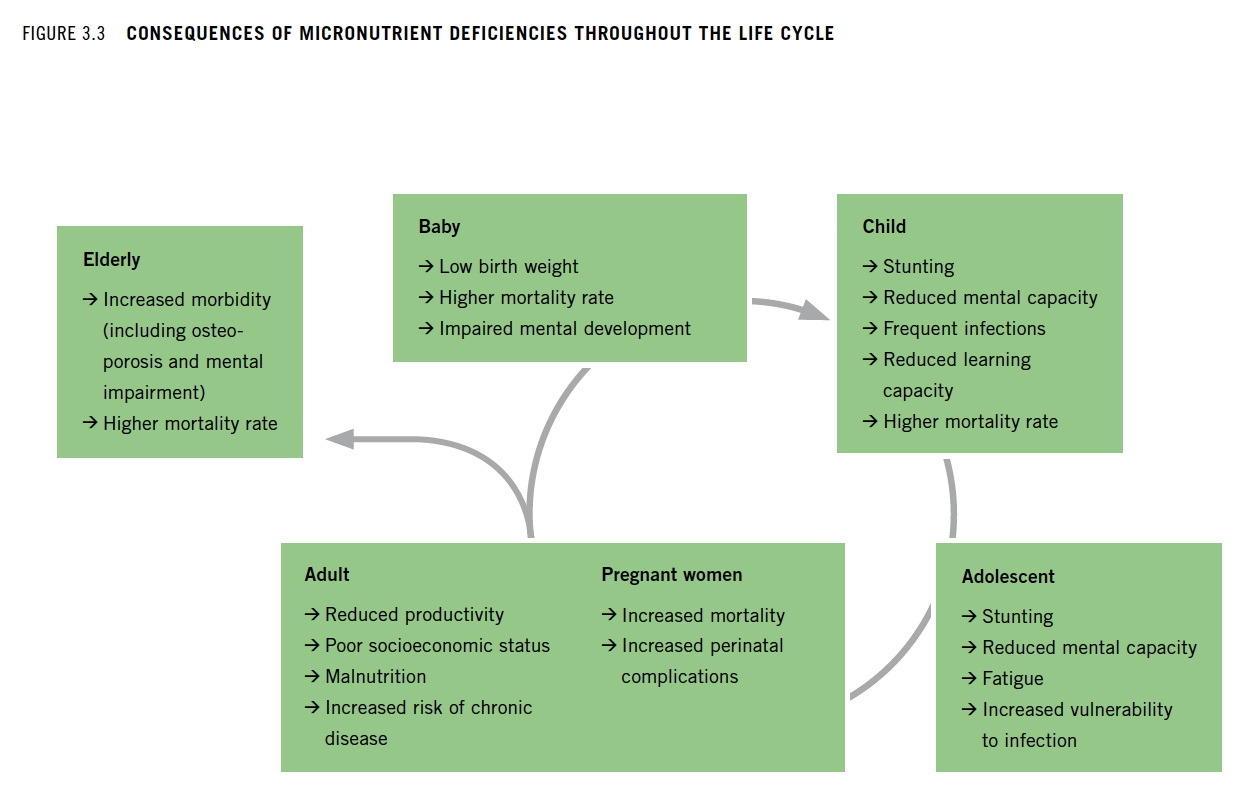
The most commonly recognized micronutrient deficiencies across all ages, in order of prevalence, are caused by a lack of iodine, iron, and zinc (Table 3.1, right). Less common, but significant from a public health standpoint, is vitamin A deficiency, with an estimated 190 million pre-school children and 19 million pregnant women affected (WHO 2009). Low intakes of other essential micronutrients, such as calcium, vitamin D, and B vitamins, such as folate are also common (Allen et al. 2006). Although pregnant women, children, and adolescents are often cited as populations affected the most by hidden hunger, it impairs the health of people throughout the life cycle (Figure 3.3, right).
It is difficult to describe the magnitude of deficits for most micronutrients. For many micronutrient deficits, prevalence data are scarce. Scientists have not reached a consensus on standard recommended intakes for many of the 19 micronutrients that directly influence physical and mental development and the immune system (Biesalski 2013). Furthermore, for many micronutrients, the relationship between intake and utilization is not well understood.
Obtaining accurate data is a challenge. Time lags, data gaps, and lack of disaggregation are common problems. Often proxies for common examples of hidden hunger are imperfect. For example, anemia is used as a proxy for iron deficiency, although only half of all anemia is caused by iron deficiency (de Benoist et al. 2008). Typical physical measurements of hunger, such as stunting (low height for one’s age), wasting (low weight for one’s height), and underweight, may capture micronutrient deficiencies in affected populations, but are inadequate proxies, because the deficiencies are seldom the only factors involved. Exact measurements via blood samples, and also by specific diagnoses, such as night blindness, beriberi, and scurvy, are more reliable ways to determine micronutrient deficiencies. Many important micronutrients lack prevalence data, because related biomarkers have not yet been identified for a nutrient deficit. As long as these gaps in data persist, it will be difficult to describe the full contours of hidden hunger.
Causes of Vitamin and Mineral Deficiencies
Box 3.2
EFFECTS OF THE GREEN REVOLUTION
Public research and development practice have over many years focused on increasing productivity of staple crops in order to reduce malnutrition. However, the intensified production of high-yielding cereal varieties during the Green Revolution from the 1970s to mid-1990s may have both improved and worsened nutrition. The increase in total output of food staples translated into a drop in the prices of starchy staples relative to the prices of more micronutrient-rich non-staple foods, such as vegetables and pulses. While staple cereals became more affordable, the prices of non-staple foods in some countries rose, making micronutrient-rich foods less attractive to poor people (Bouis 2000; Kennedy and Bouis 1993).
Poor diet is a common source of hidden hunger. Diets based mostly on staple crops, such as maize, wheat, rice, and cassava, which provide a large share of energy but relatively low amounts of essential vitamins and minerals, frequently result in hidden hunger.
What people eat depends on many factors, including relative prices (Box 3.2) and preferences shaped by culture; peer pressure; and geographical, environmental, and seasonal factors. Victims of hidden hunger may not understand the importance of a balanced, nutritious diet. Nor may they be able to afford or access a wide range of nutritious foods such as animal-source foods (meat, eggs, fish, and dairy), fruits, or vegetables, especially in developing countries. In non-emergency situations, poverty is a major factor that limits access to adequate nutritious foods.
When food prices rise, consumers tend to continue to eat staple foods while cutting their intake of non-staple foods that tend to be richer in micronutrients (Bouis, Eozenou, and Rahman 2011).
Another source of micronutrient deficiencies is impaired absorption or use of nutrients. Absorption may be impaired by infection or a parasite that can also lead to the loss of or increased need for many micronutrients. Infections and parasites can spread easily in unhealthy environments with poor water, sanitation, and hygiene conditions. Unsafe food handling and feeding practices can further exacerbate nutrient losses.
Diet also affects absorption. Fat-soluble vitamins such as vitamin A are best absorbed when consumed with dietary fat, while consumption of some compounds such as tannins or phytates can inhibit iron absorption. Alcohol consumption can interfere with the absorption of micronutrients.
The Economic Toll
Figure 3.4 Cycle of hidden hunger, poverty, and stalled development
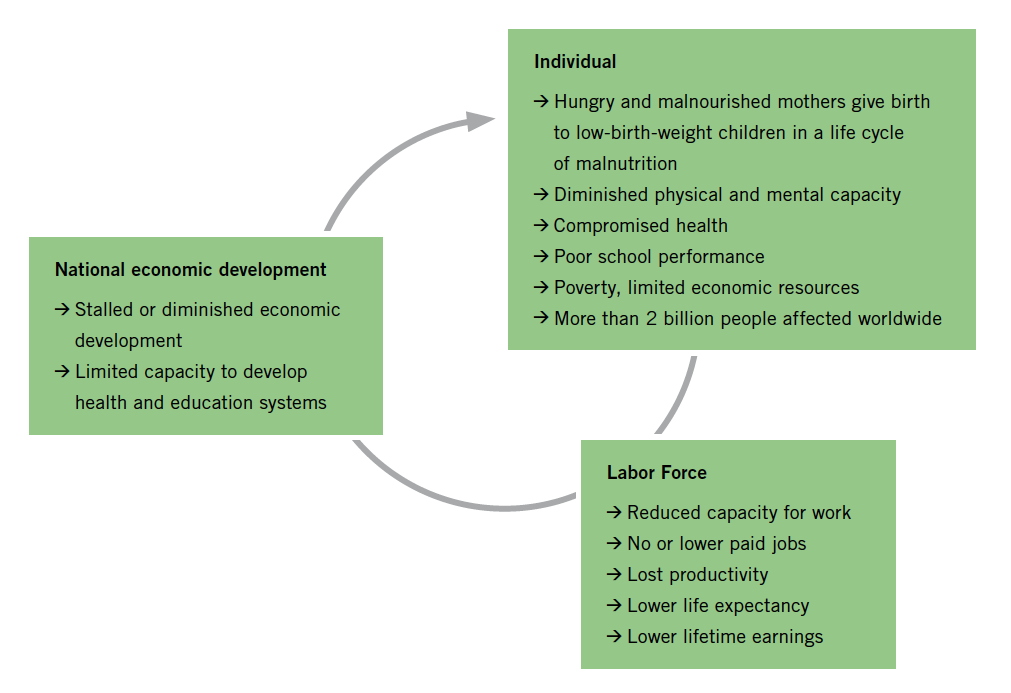 Sources: Black et al. (2013); IFPRI (2014); FAO (2013); von Grebmer et al. (2010). Note: The life cycle of malnutrition refers to how women who were poorly nourished as girls tend to give birth to underweight babies, perpetuating the cycle of undernutrition.
Sources: Black et al. (2013); IFPRI (2014); FAO (2013); von Grebmer et al. (2010). Note: The life cycle of malnutrition refers to how women who were poorly nourished as girls tend to give birth to underweight babies, perpetuating the cycle of undernutrition.
Vitamin and mineral deficiencies impose a significant burden on the affected persons and societies, both in terms of health costs and negative impacts in lost human capital and reduced economic productivity.
Hidden hunger impairs physical growth and learning, limits productivity, and ultimately perpetuates poverty (Figure 3.4) in a continuous cycle. Countries where a large share of the population is affected by vitamin and mineral deficiencies cannot realize their economic potential (Stein 2013; Stein and Qaim 2007). Poor people disproportionately suffer from micronutrient deficiencies, and bear the long-term negative effects that constrain socioeconomic development (Darnton-Hill et al. 2005).
The economic costs of all forms of micronutrient deficiency can be considerable, cutting gross domestic product by 0.7–2 percent in most developing countries (Micronutrient Initiative and UNICEF 2004). For example, it is estimated that India sustains a 1 percent loss in GDP and Afghanistan a 2.3 percent loss. Global losses in economic productivity due to macronutrient and micronutrient deficiencies reach more than 2 to 3 percent of GDP (World Bank 2006) at a global cost of US$1.4 to 2.1 trillion per year (FAO 2013).
On the other hand, the return on investment in nutrition can be high. Copenhagen Consensus Expert Panels consistently find nutrition interventions cost-effective (Copenhagen Consensus 2004, 2008, 2012). In 2008, the panel ranked supplements for children (vitamin A and zinc), fortification (iron and iodine), and biofortification among the top five best investments for economic development.
For example, estimates for salt iodization suggest that every dollar invested generates up to US$81 in benefits (Hoddinott, Rosegrant, and Torero 2012).
Solutions to Hidden Hunger
Diversifying Diets
Increasing dietary diversity is one of the most effective ways to sustainably prevent hidden hunger (Thompson and Amoroso 2010). Dietary diversity is associated with better child nutritional outcomes, even when controlling for socioeconomic factors (Arimond and Ruel 2004). In the long term, dietary diversification ensures a healthy diet that contains a balanced and adequate combination of macronutrients (carbohydrates, fats, and protein); essential micronutrients; and other food-based substances such as dietary fiber.
A variety of cereals, legumes, fruits, vegetables, and animal-source foods provides adequate nutrition for most people, although certain populations, such as pregnant women, may need supplements (FAO 2013). Effective ways to promote dietary diversity involve food-based strategies, such as home gardening and educating people on better infant and young child feeding practices, food preparation, and storage/preservation methods to prevent nutrient loss.
Fortifying Commercial Foods
Commercial food fortification, which adds trace amounts of micronutrients to staple foods or condiments during processing, helps consumers get the recommended levels of micronutrients. A scalable, sustainable, and cost-effective public health strategy, fortification has been particularly successful for iodized salt: 71 percent of the world’s population has access to iodized salt and the number of iodine-deficient countries has decreased from 54 to 32 since 2003 (Andersson, Karumbunathan, and Zimmermann 2012).
Other common examples of fortification include adding B vitamins, iron, and/or zinc to wheat flour and adding vitamin A to cooking oil and sugar. Fortification may be particularly effective for urban consumers, who buy commercially processed and fortified foods. It is less likely to reach rural consumers who often have no access to commercially produced foods. To reach those most in need, fortification must be subsidized or mandatory; otherwise people may buy cheaper non-fortified alternatives.
Fortification, however, has a number of shortcomings. People may resist fortified foods. For example, up to 30 percent of Pakistanis avoid iodized salt, according to the Micronutrient Initiative, due to a mistaken belief that iodine causes infertility and rumors of a plot to limit population growth (Leiby 2012). Consumers may also resist using fortified foods due to cooking properties or flavor. From another perspective, it can be difficult to determine the appropriate level of nutrients. Fortificants, the compounds used to fortify foods, may not be stable and may be lost during processing or storage.
In addition, bio-availability, the degree or rate at which a substance can be absorbed, may be limited. That said, evidence of the acceptability and efficacy of home fortification continues to grow (Adu-Afarwuah et al. 2008; Dewey, Yang, and Boy 2009; De-Regil et al. 2013).
Biofortification
Biofortification is a relatively new intervention that involves breeding food crops, using conventional or transgenic methods, to increase their micronutrient content. Plant breeders also improve yield and pest resistance, as well as consumption traits, like taste and cooking time—to match or outperform conventional varieties. To date, only conventionally bred biofortified crops have been released and delivered to farmers. Biofortified crops that have been released so far include vitamin A orange sweet potato, vitamin A maize, vitamin A cassava, iron beans, iron pearl millet, zinc rice, and zinc wheat.
While biofortified crops are not available in all developing countries, biofortification is expected to grow significantly in the next five years (Saltzman et al. 2013).
Biofortified foods could provide a steady and safe source of certain micronutrients for people not reached by other interventions. In contrast to large-scale fortification, which usually reaches a greater share of urban than rural residents, biofortification first targets rural areas where crops are produced. Marketed surpluses of biofortified crops may make their way into retail outlets, reaching consumers first in rural areas, then in urban ones.
Given that biofortified staple foods cannot deliver as high a level nor as wide a range of minerals and vitamins as supplements or industrially fortified foods can, they are not the best response to clinical deficiencies. However, they can help close the micronutrient intake gap and increase the daily intake of vitamins and minerals throughout a person’s life (Bouis et al. 2011). While the evidence on biofortification is not yet complete, several crops (iron beans, maize, pearl millet, rice, sweet potato, and vitamin A cassava) show evidence of improved micronutrient levels (Haas et al. 2005; 2011; 2013; 2014; Luna et al. 2012; Scott et al. 2012; Pompano et al. 2013; De Moura et al. 2014; Tanumihardjo 2013; Talsma 2014; van Jaarsveld et al. 2005). Interventions delivering biofortified orange sweet potato significantly improved vitamin A intake of mothers and young children (Hotz et al. 2012a; Hotz et al. 2012b).
Supplementation
Vitamin A supplementation is one of the most cost-effective interventions for improving child survival (Tan-Torres Edejer et al. 2005). Between 1999 and 2005, coverage increased more than fourfold, and in 2012, estimated coverage rates were near 70 percent globally (UNICEF 2014b). Programs to supplement vitamin A are often integrated into national health policies because they are associated with a reduced risk of all-cause mortality and a reduced incidence of diarrhea (Imdad et al. 2010). According to UNICEF, at least 70 percent of young children ages 6 to 59 months need to receive vitamin A supplements every six months in order to achieve the desired reductions in child mortality. However, because of fluctuations in funding, coverage varies widely from year to year in many priority countries.
It should also be noted that vitamin A supplements typically target only vulnerable populations between six months and five years old. Supplementation for other micronutrient deficiencies is less common. In some countries, iron-folate supplements are prescribed to pregnant women though coverage rates are often low and compliance rates even lower. For children, home fortification with micro-nutrient powders and lipid-based nutrient supplements can include multiple micronutrients, like iron and zinc, but they are harder to get into homes on a large scale than vitamin A supplements.
The learning curve can be steep. In a trial in rural China, about half of parents or grandparents stopped giving children nutritional supplements containing soybeans, iron, zinc, calcium, and vitamins because they suspected the free supplements were unsafe or fake. They also feared they would be charged later (Economist 2014).
Looking Ahead
A range of interventions are needed to solve the complex problem of hidden hunger. To sustainably tackle the underlying causes will require a multisectoral approach at the national and international levels.
National governments must take a cohesive approach to confronting hidden hunger, otherwise it will not get the attention it deserves. Only when all ministries, including agriculture, health, child development, and education, and those handling regulatory affairs, form a united front to improve food and nutrition security will governments truly have a chance of succeeding.
The Scaling Up Nutrition (SUN) Movement offers a model for cross-sectoral collaboration, bringing people and resources together at the national level to improve nutrition (SUN 2014). Essential components to fight hidden hunger must include:
-
Behavior-change communication that aims to improve women’s, infants’, and young children’s utilization of health services, clean water, good sanitation, and hygiene to protect them from diseases that interfere with nutrient absorption;
-
Messaging that promotes best practices, such as early initiation of exclusive breastfeeding up to 6 months followed by breastfeeding up to 24 months with adequate and sufficient complementary food as an economic and sustainable way to prevent hidden hunger in children;
-
Social protection that gives poor people access to nutritious food and shields them from price spikes; and
-
A focus on empowering women by increasing access to education.
Eliminating hidden hunger will not be easy. Challenges lie ahead. But if enough resources are allocated, the right policies developed, and the right investments made, these challenges can be overcome (Fan and Polman 2014). Much still needs to be done to ensure that people around the world gain access to the nutrient-rich foods they and their communities need to combat poor health and reach their development potential.
Footnotes
- Conventional plant breeding involves parent lines with high vitamin or mineral levels that are crossed over several generations to produce plants with the desired nutrient and agronomic traits. Transgenic approaches, in which genes are manipulated or new genes inserted, are advantageous when the nutrient is not naturally found in a crop (for example, provitamin A in rice).