Haiti
A Closer Look at Hunger and Undernutrition
MAP OF HAITI
 Note: Haiti is divided into 10 departments. Aire Métropolitaine, which contains the capital,
Port-au-Prince, as well as other urban areas, is part of Ouest department.
Note: Haiti is divided into 10 departments. Aire Métropolitaine, which contains the capital,
Port-au-Prince, as well as other urban areas, is part of Ouest department.
Haiti, located on the western side of Hispaniola Island, which it shares with the Dominican Republic in the Caribbean Sea, has experienced substantial challenges in recent decades, including multiple coups, devastating natural disasters, and persistent poverty (Taft-Morales 2017). Haiti has a poverty rate of 25 percent according to the most recent official statistics, which date from 2012. Its GDP per capita was just $766 as of 2017—less than one-tenth of the average for Latin America and the Caribbean—and has grown at a rate of less than 0.5 percent a year on average since 2010 (World Bank 2019a). The country has undergone rapid urbanization since the 1950s, yet its cities are beset by high levels of poverty and lack the infrastructure and services to successfully accommodate their growing populations (Lozano-Gracia and Lozano 2017).
Agriculture plays an important role in the Haitian economy, representing half of total employment, while 40 percent of employment is in services and 10 percent in industry. Agriculture contributes 18 percent of GDP, services 23 percent, and industry 57 percent (World Bank 2019a). The majority of farmers operate small-scale subsistence farms and have access to less than two hectares of land (FEWS NET 2015). The agricultural sector is important for Haitians’ livelihoods and food and nutrition security, but it is plagued by environmental degradation, soil erosion, underinvestment, and low productivity (Duvivier and Fontin 2017). Women play a critical role in Haitian agriculture, yet they experience inequitable treatment; for example, they lack the same land inheritance rights as men and receive lower wages for agricultural work (Tandon 2012).
Haiti is extremely vulnerable to the effects of climate change and is poorly equipped to implement solutions to adapt to these effects. Like other small island developing states, Haiti is particularly vulnerable to rising sea levels, extreme weather events such as hurricanes, and storm surges (UNDP 2017; Gallagher et al. 2019). Haiti’s urban and rural areas face distinct challenges and circumstances as the result of climate change. The positioning of Haiti’s cities—on the coast, on riverbeds, and on hillsides—increases their vulnerability to flooding and landslides, while deforestation and poor soil quality leave the Haitian countryside ill prepared to deal with worsening climatic conditions (Rubenstein 2012). In both urban and rural areas, poverty, low levels of education and literacy, and inadequate infrastructure exacerbate the population’s vulnerability to the impacts of climate change (CAF 2014).
In the past 10 years, Haiti has been affected by multiple catastrophic disasters. In 2010, a 7.0-magnitude earthquake hit near its capital, Port-au-Prince, killing 230,000 people, injuring 300,000, and causing massive damage to infrastructure (Dupuy 2010). Later that year, a large-scale cholera epidemic spread throughout the country. Still not completely eradicated, cholera infected 819,000 people and resulted in nearly 10,000 deaths between 2010 and 2018 (UN OCHA 2019b). Hurricane Sandy in 2012 and Hurricane Matthew in 2016 further damaged the country, including the agricultural sector (FAO 2019c). In 2018, drought conditions in the north of the country delayed the harvest and exacerbated food insecurity (CARE International 2019). In 2019, political unrest, substantial inflation, and continued drought in some parts of the country have magnified the ongoing threats the population is facing (ACF 2019).
Cumulatively, these challenges amount to a massive humanitarian crisis, with 2.6 million Haitians out of a population of approximately 11 million estimated to be in need of humanitarian assistance in 2019 (CARE International 2019; World Bank 2019a). Even so, the situation has gone largely unnoticed, earning it the distinctions of being the most underfunded and the most underreported humanitarian crisis in 2018 (CARE International 2019; UN OCHA 2019c).
Hunger and Undernutrition in Haiti
HAITI’S GLOBAL HUNGER INDEX SCORES AND INDICATOR VALUES, 2000, 2005, 2010, AND 2019
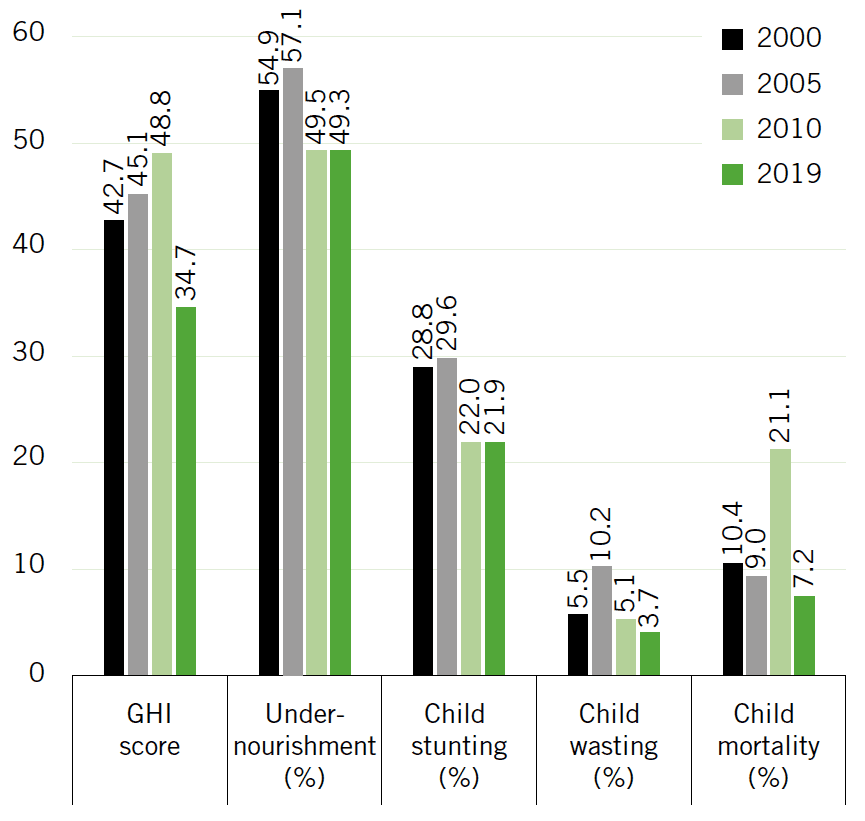
Note: Undernourishment values refer to the prevalence of undernourishment for the country’s population as a whole; child stunting, child wasting, and child mortality refer to the rates for each indicator for children under the age of five. Data for GHI scores, child stunting, and child wasting are from 1998–2002 (2000), 2003–2007 (2005), 2008–2012 (2010), and 2014–2018 (2019). Data for undernourishment are from 1999–2001 (2000), 2004–2006 (2005), 2009–2011 (2010), and 2016–2018 (2019). Data for child mortality are from 2000, 2005, 2010, and 2017 (2019). See Appendix A for the formula for calculating GHI scores and Appendix B for the sources from which the data are compiled.
Since 2000, Haiti’s progress on reducing hunger and undernutrition has been uneven. Its 2005 GHI score was higher than that from 2000, and its 2010 score was higher still, indicating an increase in hunger and undernutrition, yet its 2019 score declined to 34.7, the lowest value observed in the time series since 2000. This latest score, however, is still at the very high end of the serious category on the GHI Severity Scale and is the seventh-highest 2019 GHI score among all countries in this report for which adequate data are available to calculate scores.
Haiti’s high score is driven mainly by its undernourishment rate, which is the third-highest value in this year’s report (see Appendix C). At 49.3 percent, Haiti’s 2016–2018 undernourishment rate is nearly the same as it was in 2009–2011 (49.5 percent), showing that approximately half of the population is not able to meet its minimum calorie requirements on a regular basis (Figure 4.4). Key contributors to food insecurity in Haiti include a high poverty rate and low agricultural productivity, which, in turn, results from frequent natural disasters, a high level of environmental degradation, and heavy reliance on rain-fed agriculture (USAID 2017).
Many Haitians consume poor-quality diets with low dietary diversity. According to a countrywide assessment, iron-rich foods were lacking in the diets of half of households, and at least one in four households had deficits in the consumption of foods rich in protein and vitamin A (WFP 2016). A small-scale study in southwestern Haiti found that fish, meat, dairy, and eggs, which are rich in protein and micronutrients, were the least frequently consumed food groups. Pulses and nuts, which are also good sources of protein and micronutrients, were more frequently consumed, but more than one-third of households had not consumed any fruits or vegetables the previous day (Pauzé et al. 2016). Rice, maize, wheat, and sorghum are the most highly consumed cereals. Haitians also regularly consume roots and tubers (mainly sweet potatoes, cassava, and yams), plantains, beans, and peas. The country is dependent on imports of rice, wheat, and edible oils. Rice consumption and a dependence on rice imports have increased considerably since the 1980s, when Haiti dramatically reduced its tariffs on imported rice (FEWS NET 2018).
Haiti experienced a steady decline in its child mortality rate for decades before 2010, when the rate spiked dramatically owing to deaths by injury from the earthquake that occurred in that year (Liu et al. 2012). In 2011, the rate went back to its previous trajectory and continued to decline. Nonetheless, at 7.2 percent, Haiti’s child mortality rate is still the highest in the Western Hemisphere (UN IGME 2018). Although a comprehensive explanation for the decline in child mortality is not available, recent factors have likely included the Soins Obstétricaux Gratuits and Soins Infantiles Gratuits programs— introduced in 2008 and 2010, respectively—which provide free access to health care for pregnant women and newborns and for children under the age of five (Amibor 2013).
The most recent data show Haiti’s child stunting rate at 21.9 percent, which is considered high in terms of its public health significance, while its child wasting rate, at 3.7 percent, is considered low (IHE and ICF 2018; de Onis et al. 2019). There is some variation at the subnational level, with the highest stunting rate in the Centre department, recorded at 30.1 percent, and the highest wasting rate in Aire Métropolitaine, the greater Port-au-Prince metropolitan area, recorded at 5.9 percent (Table 4.2). Remarkably, according to survey data from 2012 and 2016–2017, Haiti’s child undernutrition levels are lower than they were in 2005–2006, before the 2010 earthquake. This result likely reflects the extensive humanitarian efforts undertaken after the earthquake, including various strategies designed specifically to combat child undernutrition (Ayoya et al. 2013). Still, additional efforts are needed to improve children’s diets and nutritional status. In Haiti just 40 percent of children under 6 months of age are exclusively breastfed, and just 11 percent of children ages 6 to 23 months received a minimum acceptable diet (IHE and ICF 2018). A study conducted in an informal urban settlement in Haiti found that poverty, household food insecurity, time constraints, women’s employment, and limited social support were associated with low rates of exclusive breastfeeding (Lesorogol et al. 2018).
There is evidence that poor water, sanitation, and hygiene conditions compromise children’s nutritional status, most likely through negative impacts on their health and their ability to properly absorb nutrients (Fink, Günther, and Hill 2011; Ngure et al. 2014). Children in Haiti with access to an improved water source and sanitation services are less likely to be stunted than children with comparable diets and care who do not have the same access to water and sanitation (World Bank 2017a). In Haiti just 31 percent of households have access to improved toilet facilities, while an additional 24 percent have access to facilities that would be considered improved if they were not shared, and 25 percent of households have no toilet facilities at all. In surveyed households where the location most commonly used for hand washing was observed, 60 percent did not contain water, soap, or other hand-washing products. Meanwhile, 74 percent of households have access to improved drinking water sources (IHE and ICF 2018).
HIV/AIDS, which affected approximately 2 percent of the Haitian population aged 15–49 years as of 2017 (CDC 2019), is associated with food insecurity and undernutrition. The links go two ways: HIV/ AIDS can worsen food security and nutrition status, and low food security and poor nutrition can, in turn, worsen the effects of HIV/ AIDS (Ivers et al. 2010). A study of HIV-positive adults in rural areas of Artibonite department in 2010/2011 found that 51 percent of those surveyed were severely food insecure, an additional 38 percent were moderately food insecure, and the severely food insecure had particularly low dietary diversity (Rebick et al. 2016).
Interventions That Affect Food Insecurity and Undernutrition
Table
GHI INDICATOR VALUES BY DEPARTMENT, HAITI
| Department | Child stunting (%) | Child wasting (%) | Child mortality (%) |
|---|---|---|---|
| Aire Métropolitainea | 20.2 | 5.9 | 8.9 |
| Ouestb | 22.5 | 3.6 | 11.2 |
| Sud-Est | 20.0 | 2.5 | 7.6 |
| Nord | 20.0 | 3.6 | 5.4 |
| Nord-Est | 21.0 | 1.5 | 7.7 |
| Artibonite | 22.4 | 4.3 | 8.4 |
| Centre | 30.1 | 2.9 | 9.0 |
| Sud | 22.0 | 2.9 | 6.2 |
| Grande Anse | 21.6 | 3.4 | 5.3 |
| Nord-Ouest | 20.3 | 2.4 | 5.8 |
| Nippes | 17.2 | 3.6 | 9.0 |
| Total | 21.9 | 3.7 | 8.3 |
|
Source: IHE and ICF (2018). Note: All indicators are for children under five years of age. Undernourishment values at the subnational level are not currently available for Haiti. The national child mortality estimates here and in Figure 4.4 differ because IHE and ICF (2018), which contains subnational values for the 10 years preceding the survey in 2016–2017, is cited here and was used by the authors to calculate the national total, while UN IGME (2018), which includes estimates for individual calendar years, is cited in Figure 4.4 and is used to calculate the GHI scores. a Aire Métropolitaine consists of the urban areas of six municipalities in Ouest department: Port-au-Prince, Tabarre, Cité Soleil, Carrefour, Delmas, and Pétion-Ville. b The values given here are for the Ouest department outside of Aire Métropolitaine. |
|||
Researchers have conducted a range of studies to assess the effectiveness of efforts to reduce hunger and undernutrition. The following is a selection of studies demonstrating the types of interventions that have been shown to reduce hunger, undernutrition, or both in the context of Haiti. Unlike many countries for which there is a substantial body of research documenting the impacts of nutrition-sensitive interventions, such as agriculture or cash transfer programs, the existing literature for Haiti is primarily focused on nutrition-specific interventions, such as providing nutritional supplements to children or food assistance to adults. Additional research is needed to determine which types of nutrition-sensitive programs are effective in Haiti and which ones could successfully be implemented at scale.
A maternal and child health and nutrition program implemented in the Central Plateau of Haiti provided preventative health services and food assistance to pregnant and lactating women and children and behavior change communication to mothers. Monthly food rations for children and behavior change communication to mothers of young children were provided either on a preventative basis (targeted to all children aged 6–23 months) or recuperative basis (targeted to children aged 6–59 months who were determined to be already undernourished). In the preventative program, behavior change communication included child feeding and care practices to prevent undernutrition; in the recuperative program, it included causes of undernutrition, nutritious recipes, feeding during illness, and hygiene in food preparation, handling, and storage. Children in both program groups had lower stunting rates than children in a matched control group (Donegan et al. 2010), while the preventative approach was more effective at reducing child stunting, wasting, and underweight than the recuperative approach (Ruel et al. 2008). Another evaluation stemming from the same program compared methods for treating anemia in young children aged 9–24 months. One group of children received an iron-fortified wheat-soy blend ration, and the other group received the same ration plus a supply of micronutrient Sprinkles—sachets containing micronutrients in powdered form that can be added to common foods—over a period of two months. In the group that received the Sprinkles, anemia prevalence fell by more than half (from 54 to 24 percent), whereas in the other group anemia prevalence increased slightly, showing that the iron-fortified wheat-soy blend alone was insufficient to reduce anemia in anemic young children (Menon et al. 2007).
In 2011–2012 children aged 6–11 months living in an informal urban settlement in Cap-Haïtien were given a daily lipid-based nutrient supplement for a duration of either three or six months. Those who received the supplement for six months experienced greater linear growth than the control group, which received no supplementation until after the study period (Iannotti et al. 2013). A related study implemented in 2013—also in Cap Haïtien—evaluated a school feeding program for children aged 3–13 years that was implemented over a period of 100 days. Students received either a fortified peanut butter paste, a nonfortified cereal bar, or no supplementation at all during the trial. Relative to the other groups, those who received the fortified paste had a lower risk of developing anemia and showed increased body mass index and fat mass—a positive result given that thinness was common among these Haitian schoolchildren (Iannotti et al. 2015).
Several studies have explored food and nutrition interventions targeted at the population living with HIV/AIDS. A study of a Partners in Health program implemented in central Haiti showed that combining food assistance with comprehensive healthcare improved food security, increased body mass index, and strengthened adherence to clinic visits among patients with HIV more so than healthcare alone (Ivers et al. 2010). Further experimentation showed that there was no statistically significant difference in these outcomes whether the beneficiaries received a ready-to-use supplementary food (fortified peanut paste) or a less expensive fortified corn-soybean blend (Ivers et al. 2014). A study implemented in Port-au-Prince in 2008–2009 as part of a prevention of mother-to-child transmission (PMTCT) program provided nutrition support to HIV-exposed, uninfected, non-breastfed children aged 6–12 months with HIV-positive mothers over the course of 24 weeks. Program components included a lipid-based nutrient supplement for the children; behavior change education regarding infant feeding, hygiene, and diarrhea treatment; promotion of existing clinical services; and social support. The children in the program had lower stunting and underweight rates than children in a comparable control group (Heidkamp et al. 2012).
The types of interventions covered by these impact evaluations may not perfectly reflect the full scope of the programs that have been implemented in Haiti. However, the focus on child nutrition programs in the literature, combined with Haiti’s extraordinarily high undernourishment rate and more moderate child stunting and wasting rates, suggests that food production and food access have received less attention than children’s nutrition in recent years. The Haitian government and the international community must increase resources and interventions to focus on persistent shortcomings related to children’s diets and nutrition while also addressing broader societal issues that are currently limiting food and nutrition security for the population as a whole.
Existing Policies and Government Measures Affecting Food Security and Nutrition
-
The Constitution of Haiti (1987) establishes the right to food as fundamental: “The State recognizes the right of every citizen to decent housing, education, food and social security” (GoH 1987).
-
The Ministry of Agriculture, Natural Resources and Rural Development is the primary institution responsible for improving food and nutrition security, while the Ministry of Public Health and Population is principally tasked with nutrition-related services (Duvivier and Fontin 2017). However, the abolition of the National Commission for Hunger and Malnutrition in 2014 weakened the perceived position of food and nutrition security on the political agenda (SUN 2017a).
-
Haiti’s Strategic Development Plan (2012–2030; Plan Stratégique de Développement d’Haïti, PSDH) acknowledges that the level of food insecurity is high and that action must be taken in multiple areas to address the problem (GoH 2012).
-
The National Nutrition Policy (2012; Politique Nationale de Nutrition, PNN) aims to improve the nutrition and health status of the population and of vulnerable groups, including pregnant women, lactating women, and children under five years of age (Duvivier and Fontin 2017).
-
The Nutrition Strategic Plan (2013–2018) sought to improve the health and nutritional status of the population, including vulnerable groups, by prioritizing the following areas: preventing malnutrition, addressing nutrition-related diseases, protecting nutrition in case of emergencies, improving information systems for nutrition, improving intersectoral and intra- and inter-ministerial coordination, and providing applied research and training in the field of nutrition (GoH 2013; FNSP 2019).
-
The Food Security and Nutrition Programme, launched in 2019, is a collaboration between the Government of Haiti and the European Union. Focused on the Nord-Ouest, Haut Artibonite, and Grande Anse departments, the program aims to sustainably improve the food security and nutrition of the most vulnerable populations and develop their resilience and capacity to resist and overcome shocks and crises (SUN 2019).
-
Haiti ratified the Paris Agreement and introduced the National Climate Change Policy (Politique Nationale de Lutte contre les Changements Climatiques, PNCC) in 2017. The vision of the PNCC is to reduce Haiti’s vulnerability to climate change by adopting and implementing appropriate adaptation and mitigation measures (NAP-GSP 2018). Haiti has also developed a National Action Plan on Climate Change Adaptation (FAO 2019c).
-
The general objective of the Agricultural Development Policy (2010–2025) is to sustainably satisfy the food needs of the population and contribute to the social and economic development of the country. Specific long-term goals include reducing the dependence on food imports and meeting the national demand for food predominantly from domestic production, creating employment opportunities in rural areas to curb migration to the cities, increasing the contribution of the agricultural sector to foreign currency earnings, and reducing environmental vulnerability (GoH 2011).
Policy and Institutional Recommendations for Moving Forward
-
Increased investment in agriculture is needed to raise productivity, increase domestic food production, and improve food and nutrition security. Additional emphasis on nutrition is required to ensure that the agricultural sector not only increases its levels of food production, but also maximizes its contribution to meeting the population’s nutrition needs. Furthermore, given the important role that women play in agriculture in Haiti, additional efforts are needed to ensure that they have access to agricultural services such as extension and financing (Duvivier and Fontin 2017).
-
Given Haiti’s extraordinarily high level of deforestation and its resulting vulnerability to flooding, landslides, and erosion, reforestation initiatives must be prioritized. Reforestation is currently underfunded, even among donor-financed climate change mitigation and adaptation initiatives. To reduce the incidence of tree cutting to meet household energy needs, increased access to alternative fuel sources is vital (FAO 2018a; Gallagher et al. 2019).
-
Improvements to the water, sanitation, and hygiene environment are necessary. Current public investments in water and sanitation services disproportionately benefit wealthy residents in urban areas. A shift of resources to benefit the poor in both urban and rural areas is therefore critical. Moreover, with the private sector providing a large proportion of water and sanitation services, increased and improved government regulation of private entities is needed (World Bank 2017a).
-
Further action is needed to improve breastfeeding practices and infant and young child feeding practices. For example, Haiti has not implemented the International Code of Marketing of Breastmilk Substitutes, which incorporates legal measures to protect the public from aggressive marketing of breast-milk substitutes. Adopting such measures is an important step the government should take, just as other countries in the region and around the world have done (SUN 2018a). Improved messaging is also necessary to correct several common misunderstandings regarding breastfeeding and complementary feeding for infants and young children (Laterra et al. 2014). In addition, the provision of childcare at or near women’s workplaces could support mothers’ ability to breastfeed, while economic support such as cash transfers could reduce the need for mothers to work outside the home during the first six months—the period when exclusive breastfeeding is recommended (Lesorogol et al. 2018).
-
While considerable international funds have been invested in climate-specific or climate-related projects, multiple areas that have been prioritized by the Haitian government remain unfunded or underfunded, such as coastal resilience and coastal zone management, agricultural adaptation, and institutional strengthening and capacity building. To maximize scarce resources, the government and international donors are advised to mainstream climate change action into development strategies and disaster risk reduction activities (Gallagher et al. 2019). Investments are desperately needed to strengthen resilience and to help communities adapt their livelihoods and withstand weather- and climate-related shocks.
Footnotes
- This rate reflects the share of the population living on less than $1.90 a day (based on 2011 purchasing power parity).
- GDP per capita is expressed in current US dollars.
- Haiti ranks 173rd out of 181 countries on the Notre Dame Global Adaptation Initiative (ND-GAIN) index, which summarizes countries’ vulnerability to climate change in combination with their readiness to improve their resilience (ND-GAIN 2019).
- The high 2010 score can be attributed in part to the abnormally high child mortality rate that year, resulting largely from the 2010 earthquake (Liu et al. 2012).
- There are 22 countries with higher child mortality rates in this report, 55 countries with higher stunting rates, and 71 countries with higher wasting rates (see Appendix C).
- Studies were considered for inclusion in this section if they evaluated the effect of an intervention on diet or nutrition using a suitable control group for comparison.