Malawi
A Closer Look at Hunger and Undernutrition
Progress Despite Formidable Challenges
FIGURE 1: MAP OF MALAWI
1. Blantyre
2. Chiradzulu
3. Phalombe
4. Mulanje
5. Thyolo
Despite facing many challenges, Malawi has made notable progress since 2000 in reducing its overall hunger and undernutrition levels as measured by the Global Hunger Index. This report gives a brief overview of Malawi’s economic situation, describes its hunger and undernutrition status, reviews the types of programs that have been shown to affect food and nutrition security, and highlights existing policies and policy recommendations aimed at achieving further progress.
Malawi is a small, land-locked country with an area of just under 120,000 square kilometers, or 46,000 square miles. Of this area, approximately 20 percent is covered by water, including the massive Lake Malawi, which lies along the country’s eastern border (World Atlas 2017). Malawi is divided into three regions: the least-populated Northern region; the Central region, home to the capital, Lilongwe; and the Southern region. The country is peaceful, and its government is relatively democratic and stable (World Bank 2018).
The most recent official poverty statistics for Malawi show that as of 2010, 71.4 of the population lived in poverty, only marginally lower than in 2004 when the poverty rate was 72.8 percent (World Bank 2019). World Bank projections suggest that this rate inched down slightly to 69.2 percent by 2017 (World Bank 2017). Malawi’s GDP per capita as of 2017 was just $338 in current US dollars. This is the second-lowest GDP per capita of all countries with available data; only Burundi is lower. Since 2010, GDP per capita has grown at an average annual rate of just 1.2 percent (World Bank 2019).
Agriculture plays a vital role in Malawi’s economy, accounting for 85 percent of employment, compared with just 7 percent in services and 8 percent in industry as of 2017 (World Bank 2019). Given the current structure of the economy, growth in Malawi’s agricultural sector is estimated to be twice as effective at reducing poverty as growth in the non-agricultural sectors (Dorosh and Thurlow 2018). At the same time, development of non-agricultural sectors is important to reduce the country’s vulnerability to extreme weather, climate change, crop failures, and commodity price fluctuations (Benfica, Squarcina, and de la Fuente 2018). Farms are predominantly rain-fed, and the agricultural sector is highly vulnerable to weather extremes (FAO 2015a), such as flooding in 2015 and drought in 2015/16, which devastated the agricultural sector (AfDB 2018). In March 2019 Cyclone Idai unleashed catastrophic flooding, affecting half of Malawi’s 28 districts. Nsanje and Chikhwawa experienced the most severe damage, including destruction of crops and livestock (MSF 2019).
Other challenges face the agricultural sector. Most landholdings are small: 73 percent of households operate less than one hectare of land (Lowder et al. 2016). The agricultural sector lacks diversification, with maize and tobacco dominating production (GoM 2016).
The country is often categorized into three main agroecological zones: the Lower Shire valley in the far south of the country; the lakeshore plains and Upper Shire valley, roughly running north to south along the eastern side of Malawi bordering Lake Malawi; and the mid-altitude plateau and highlands, predominantly along the western side of the country. Yet within these zones there is considerable diversity of climate, elevation, vegetation, water availability, market access, and population density, suggesting the importance of targeted agricultural programming (Benson, Mabiso, and Nankhuni 2016; FEWS NET 2016).
Undernourishment Persists, but Child Nutrition Is Improving
For each country, GHI scores are calculated based on values of four component indicators:
- UNDERNOURISHMENT: the share of the population that is undernourished (that is, whose caloric intake is insufficient);
- CHILD WASTING: the share of children under the age of five who are wasted (that is, who have low weight for their height, reflecting acute undernutrition);
- CHILD STUNTING: the share of children under the age of five who are stunted (that is, who have low height for their age, reflecting chronic undernutrition); and
- CHILD MORTALITY: the mortality rate of children under the age of five (in part, a reflection of the fatal mix of inadequate nutrition and unhealthy environments).
FIGURE 2: MALAWI’S GLOBAL HUNGER INDEX SCORES AND INDICATOR VALUES, 2000, 2005, 2010, AND 2018
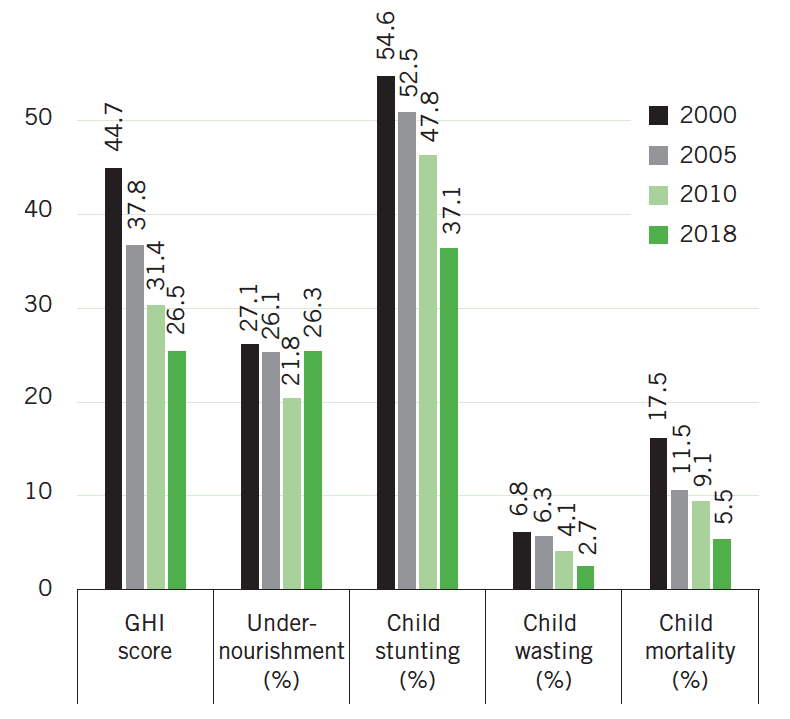
Note: Undernourishment values refer to the prevalence of undernourishment for the country’s population as a whole; child stunting, child wasting, and child mortality refer to the rates for each indicator for children under the age of five. Data for GHI scores, child stunting and child wasting are from 1998–2002 (2000), 2003–2007 (2005), 2008–2012 (2010), and 2013–2017 (2018). Data for undernourishment are from 1999–2001 (2000), 2004–2006 (2005), 2009–2011 (2010), and 2015–2017 (2018). Data for child mortality are from 2000, 2005, 2010, and 2016 (2018). See Appendix A in the 2018 GHI report for the formula for calculating GHI scores and Appendix B for the sources from which the data are compiled.
Malawi’s 2018 GHI score is 26.5, considered serious, down from 44.7 in 2000, when it was categorized as alarming. Underlying this improvement are reductions in three of the four indicator values used to calculate the GHI: child stunting, child wasting, and child mortality (Figure 2). Given the importance of child nutritional status for well-being from birth through adulthood, Malawi’s progress in this area is notable. In contrast, Malawi’s undernourishment rate—the prevalence of the population with inadequate access to calories—decreased modestly between 2000 and 2010 but has since increased, nearly erasing previous progress.
While it may seem counterintuitive that children’s nutritional status has improved despite lack of comparable progress on undernourishment for the population as a whole, children’s nutritional status is influenced by a variety of distinct factors, including inadequate intake of food in terms of either quantity or quality, poor utilization of nutrients due to infections or other illnesses, or a combination of these. These, in turn, are caused by a range of other factors, including household food insecurity; inadequate maternal health or childcare practices; or inadequate access to health services, safe water, and sanitation. The following sections thus consider the food and nutrition security situation of Malawi’s population as a whole and then that of its children, including the conditions that have contributed to recent developments.
Food Security in Malawi
Malawi’s undernourishment rate has fluctuated over the two decades since 1999–2001 (Figure 2). Between 2004–2006 and 2007–2009 it underwent a period of decline, but increased between 2013–2015 and 2015–2017 (FAO 2018), coinciding with the 2015 flooding and 2015/16 drought that crippled the agricultural sector in Malawi and beyond. This trend is also reflected in the latest Integrated Household Survey (IHS), which show food insecurity increasing between 2010/11 and 2016/2017 (NSO 2017).
The Malawian diet consists largely of staples, primarily maize, as well as rice and cassava. Most Malawians consume foods rich in micronutrients and/or protein, such as fruits, vegetables, and animal-source foods, in limited quantities (GoM 2018b; Aberman, Meerman, and Benson 2018). The Government of Malawi has prioritized maize production since at least the mid-1970s (Dorward, Chirwa, and Jayne 2011). In 2005/06, the government instituted the well-known Farm Input Subsidy Program, with the goals of increasing maize production, promoting household food security, and enhancing rural incomes (Lunduka, Ricker-Gilbert, and Fisher 2013). Even with this program, the country occasionally faces years when it produces insufficient maize for its own consumption. Also, some segments of the population have inadequate access to calories even in years when there is a surplus of maize (FAO 2015b, 2018).
Weather shocks such as droughts, floods, and high temperatures frequently decrease food production and increase food insecurity in Malawi, in part because of the difficulties of implementing food price and food stock policies to effectively mitigate these challenges (Minot 2010). Temperatures that exceed seasonal averages push down food consumption and caloric intake by decreasing food production and raising food prices. Disaggregated results show that this effect is most significant for households where the land is managed solely by women in parts of the country where land inheritance is patrilineal, perhaps because women with insecure land tenure are less likely to invest in agricultural technologies that could mitigate the effects of weather shocks (Asfaw and Maggio 2018).
Gender is an important determinant of food security in Malawi. While data on the intrahousehold distribution of food are largely lacking (and thus the extent to which women and men or girls and boys have equitable access to food is not well understood), there is evidence that female-headed households generally have poorer food security than male-headed households in Malawi (Kakota et al. 2015; Kassie et al. 2015). In the context of farming households, this is not only because female-headed households have fewer resources with which to work (such as land, education, inputs, and training), but also because the returns to the same level of resources are lower for female-headed households than for male-headed ones, suggesting they face multiple forms of discrimination (Kassie et al. 2015).
Malawi’s high prevalence of HIV/AIDS, currently at 10.6 percent of adults aged 15–64 years (corresponding to about 900,000 Malawians living with HIV), has also contributed to malnutrition and hunger in Malawi. HIV reduces the body’s ability to utilize nutrients and people’s capacity to produce or access adequate food (MoH 2017; Nyantakyi-Frimpong et al. 2016).
Improvements are necessary in not only the quantity but also the quality of people’s diets (Aberman, Meerman, and Benson 2018). Diet and nutritional status are influenced by the types of foods that households can either produce themselves or purchase from markets. The variety of crops grown on farms has been shown to be positively related to household dietary diversity and intakes of calories and protein in Malawi (Jones 2017; Koppmair et al. 2017). Studies also link crop diversity with households’ access to important micronutrients: iron, folate, vitamin A, and zinc (Jones 2017; Mazunda, Kankwamba, and Pauw 2018). In some contexts, access to markets for buying and selling food and produce influences dietary diversity more than crop choice does (Koppmair et al. 2017).
Children’s Diet and Nutrition
Malawi’s rates of child stunting (low height-for-age) and child wasting (low weight-for-height) have fallen substantially since 2000, according to the most recent data. Its child wasting rate declined from 6.8 percent in 2000 to 2.7 percent — considered “low” — in 2015–2016. At 37.1 percent in 2015–2016, Malawi’s child stunting rate was still considered “very high,” but it declined impressively relative to its 2000 rate of 54.6 percent (NSO and ORC Macro 2001; NSO and ICF 2017; de Onis et al. 2018). This improvement is likely due to reductions in childhood illnesses that inhibit the utilization of nutrients, the scaling up of direct nutrition interventions, and underlying factors such as economic growth. Nutrition programs included expansion of vitamin A supplementation and deworming for children, the promotion of proper nutrition during pregnancy and adequate infant and young child feeding practices, and the nationwide implementation of community-based treatment of children with severe acute malnutrition (Kanyuka et al. 2016).
Malawi’s mortality rate among children under age five decreased between 2000 and 2016 from 17.5 to 5.5 percent (UN IGME 2017). Analysis shows this improvement can be attributed to treatment for diarrhea, pneumonia, and malaria; insecticide-treated bed nets; vaccines; reductions in wasting and stunting; facility birth care; and prevention and treatment of HIV. These in turn were made possible by increased funding for Malawi’s health sector and by policies and interventions aimed at improving child health and nutrition (Kanyuka et al. 2016). Malawi achieved the Millennium Development Goal target of reducing child mortality by two-thirds between 1990 and 2015, yet the current rate is still higher than the Sustainable Development Goal target of 2.5 percent by 2030 (UN 2018).
Infant and young child feeding practices in Malawi have shown both significant gains and recent slumps. As of 2015–2016, 61 percent of children under six months of age nationally were exclusively breastfed. This is a remarkable improvement relative to 1992, when the rate was just 4 percent, and 2000, when the rate was 44 percent. Still, it represents a decline relative to 2010, when the rate was 72 percent (NSO and ICF 2017). The improvement between 1992 and 2010 is attributed to a variety of factors, including strong government commitment to improving infant and young child feeding practices and national advocacy to increase breastfeeding knowledge (WHO 2014). The recent decline may stem from higher employment rates for women, the availability of breastmilk alternatives, and unfavorable public opinion regarding breastfeeding, among other things (Gangire 2017). Understanding these factors is important because exclusively breastfed infants under six months of age have higher length for age and weight for age than non-exclusively breastfed infants (Kuchenbecker et al. 2015). Meanwhile, just 8 percent of children between 6 and 23 months consume a minimum acceptable diet, which also represents a worsening of the situation since 2010, when this rate was 19 percent (NSO and ICF Macro 2011; NSO and ICF 2017).
Children’s nutrition in Malawi improves with the education level of the mother, particularly when the mother attains 10 or more years of education—that is, when she reaches senior secondary school or beyond. Women’s education may benefit children’s nutrition through a variety of channels, including improved feeding practices, better knowledge about health care, and economic advantages, such as increased command over household resources by mothers (Makoka and Masibo 2015).
For each of the three GHI indicators with subnational data (child stunting, wasting, and mortality), there is considerable variation at the district level, with some districts, particularly in the Central and Southern regions, standing out with higher rates (see Table 1). The Northern region has the lowest level of multidimensional poverty, which takes into account health, education, and living standards (World Bank 2016). The Northern region also fares better than the other regions in terms of several indicators related to child nutrition and health, including higher educational attainment rates of both men and women, better handwashing facilities, and a lower total fertility rate (NSO and ICF 2017).
Interventions That Affect Food Insecurity and Undernutrition
Table 1
GHI INDICATOR VALUES BY REGION/DISTRICT, MALAWI
| Region/District | Child stunting (%) | Child wasting (%) | Child mortality (%) |
|---|---|---|---|
| Northern | 35.1 | 2.1 | 5.7 |
| Chitipa | 33 | 1.2 | 5.3 |
| Karonga | 28.4 | 2.2 | 5.9 |
| Likoma | 24.6 | 3.8 | 5.7 |
| Mzimba | 38.9 | 2.7 | 5.2 |
| Nkhata Bay | 32.5 | 0.1 | 7.4 |
| Rumphi | 32.1 | 1.5 | 6.2 |
| Central | 38.2 | 2 | 8.1 |
| Dedza | 42.8 | 2.6 | 8.4 |
| Dowa | 39 | 1 | 6.4 |
| Kasungu | 36.3 | 2.4 | 6 |
| Lilongwe | 36.6 | 1.6 | 8.4 |
| Mchinji | 44 | 3.1 | 12.3 |
| Nkhotakota | 33.2 | 1.8 | 6.4 |
| Ntcheu | 41.6 | 3.5 | 8 |
| Ntchisi | 39.5 | 1.7 | 8.4 |
| Salima | 34.5 | 1.4 | 8 |
| Southern | 36.6 | 3.5 | 7.3 |
| Balaka | 32.6 | 0.6 | 8.4 |
| Blantyre | 33.2 | 3.1 | 6.7 |
| Chikhwawa | 32.6 | 4.9 | 6.2 |
| Chiradzulu | 33.2 | 6.2 | 6.8 |
| Machinga | 38.5 | 3.4 | 8.1 |
| Mangochi | 45.4 | 1.7 | 7.3 |
| Mulanje | 36.5 | 4.1 | 10.3 |
| Mwanza | 31 | 7.1 | 5.1 |
| Neno | 45.4 | 4.1 | 9 |
| Nsanje | 31.6 | 8.7 | 5.7 |
| Phalombe | 31.4 | 2.3 | 9.7 |
| Thyolo | 35.6 | 3.4 | 5.9 |
| Zomba | 36.4 | 4.6 | 5.4 |
| Total | 37.1 | 2.7 | 7.5 |
|
Source: NSO and ICF (2017). Note: All indicators are for children under five years of age. Undernourishment values at the subnational level are not currently available for Malawi. The national under-five mortality estimates here and in Figure 2 differ because NSO and ICF (2017), which contains subnational values for the 10-year period preceding the 2015/2016 survey, is cited and was here used by the authors to calculate the national total, while UN IGME (2017), cited in Figure 2, is used for the calculation of GHI scores. |
|||
Researchers have conducted a range of studies in Malawi to assess the effectiveness of efforts to reduce hunger and undernutrition. While it is beyond the scope of this report to describe each of these programs and evaluations in detail, this section provides an overview of the literature.
Nutrition education can positively influence nutrition outcomes, especially for infants and young children, if mothers are targeted. In a project in Mchinji district, female volunteers repeatedly visited mothers around the time of childbirth and provided information about the nutrition needs of infants, including breastfeeding, weaning, and complementary foods. The program was shown to improve child nutrition, household food consumption, and children’s growth, including height (Fitzsimons et al. 2016). Also, the UN Food and Agriculture Organization’s project Improving Food Security and Nutrition Policies and Programme Outreach improved children’s dietary diversity when agricultural activities were paired with an educational component regarding children’s nutritional needs, though effects on child growth were insignificant (Kuchenbecker et al. 2017).
In terms of treating malnourished children, a trial in Malawi showed that children who were treated at home with ready-to-use therapeutic food (RUTF) gained weight and recovered more quickly than children who were given standard inpatient care, including milk-based liquid food (Ciliberto et al. 2005). Another trial found that recovery rates of undernourished children who were given fortified spreads (milk/peanut and soy/peanut) were better than for those given fortified corn/soy blended flour, perhaps because the spreads were relatively energy-dense, did not require cooking, and were less likely to be shared with other family members (Matilsky et al. 2009).
Access to financial services can improve food consumption and nutrition. In Lilongwe, Mchinji, and Dedza districts in central Malawi, when trained financial services extension workers provided community members with information regarding savings accounts, the community members increased their savings account usage, investments in farms, household income, food security, and meat consumption (Flory 2016). A Village Savings and Loan Association (VSLA) program—a group-based savings program—operated by the nongovernmental organization Soldev in northern Malawi improved food consumption as measured by the number of meals consumed per day (Ksoll et al. 2016). However, another VSLA program evaluated in Mzimba, Mchinji, Lilongwe, and Zomba districts led to improvements in business outcomes and women’s empowerment but not in food security (Karlan et al. 2017). More research is needed on financial services interventions to determine what program components and magnitudes of impact are necessary to improve food security.
Cash transfer programs, commonly implemented worldwide, have been shown to successfully improve diet, but evidence of their effect on nutritional status is weak (Gitter et al. 2017). The Malawi Social Cash Transfer Programme (SCTP), an unconditional cash transfer program targeted to ultra-poor and labor-constrained households, was expected to reach at least 1.5 million beneficiaries in all 28 districts in 2018 (Kutengule 2018). The program’s midline evaluation showed that the SCTP improved food security for beneficiaries after one year of implementation according to various measures, including an increase in per capita total food and vegetable expenditures for the poorest households, an increase in the average number of meals eaten per day, and improvement of some measures of young child feeding practices depending on the size of the household (Handa et al. 2015). An additional study found that the SCTP increased calorie availability for beneficiaries as a whole, while other food and nutrition security measures such as food expenditures and household dietary diversity scores increased only for households for whom the transfers exceeded 20 percent of baseline consumption (Brugh et al. 2018). SCTP also increased investment in agricultural production, reduced children’s begging for food or money, and reduced children’s absences from school to work for food or money (Covarrubias, Davis, and Winters 2012).
In terms of agricultural programs, the Farm Input Subsidy Program (FISP), through which the government subsidizes inputs primarily for maize production, has occupied a significant proportion of the country’s agricultural budget since its introduction in 2005/06. In 2018/19, the budget for FISP was 53 percent of the total budget for the agricultural sector (UNDP 2018). The program was expected to reach 1 million beneficiaries in 2018/19 (Kujaliwa 2018). While the program is officially meant to benefit vulnerable and marginalized farmers, there have been allegations of elite capture and political influences on the selection of beneficiaries (Mdee and Dedaa 2018; Asfaw et al. 2017). Initially focused solely on fertilizer and improved maize seed, the program evolved to include seed for other crops as well (Lunduka, Ricker-Gilbert, and Fisher 2013). Evaluations have shown that FISP has led to modest increases in maize productivity, but the cost-effectiveness has been actively debated (Ricker-Gilbert, Jayne, and Shively 2013). In terms of food security, access to FISP was associated with an increase in self-reported adequacy of food consumption. FISP recipients also reported a lower incidence of child illness (Chirwa and Dorward 2013). Interestingly, FISP recipients have been shown to have higher levels of crop diversity and dietary diversity than non-FISP recipients, even when seed coupons were only redeemable for maize. Higher dietary diversity appears to be due in part to increased income that allows beneficiaries to purchase more diverse foods (Snapp and Fisher 2015).
Other agricultural interventions have also benefited food security. The Soils, Food, and Healthy Communities project, run by Ekwendeni Hospital staff and Malawian and Canadian scientists, encouraged farmers to intercrop legumes with other crops to improve soil fertility, food security, and child nutrition. The project also provided training on gender issues and children’s nutritional needs. Findings showed that the longer and more intensively villages were involved in the project, the more substantial were the improvements in children’s growth (Bezner Kerr, Berti, and Lizzie 2010). The Malawi Farmer to Farmer Agroecology project, run by the Soils, Food, and Healthy Communities organization as a follow-up to the previous project, encourages farmers to engage in experimentation and to share knowledge regarding agroecology, nutrition, social equity, and local food market development. Participating households showed increased food security, as measured by the Household Food Insecurity Access Scale, compared with the control group (Kangmennaang et al. 2017). In an evaluation of the impacts of plant-breeding programs in Malawi, adopters of improved bean varieties had household dietary diversity scores that were 15 percent higher than those of non-adopters (Katungi et al. 2017). Evaluation of the Bwanje Valley Irrigation Scheme shows that program participants had higher daily per capita calorie intake and annual agricultural income than those in control groups (Nkhata, Jumbe, and Mwabumba 2014)
With various types of interventions available for influencing food security and nutrition, it is interesting to consider the findings of Ecker and Qaim (2011). By modeling the effects of changes in income as well as changes in maize prices on micronutrient consumption in Malawi, they find that income increases are more beneficial to overall nutrition than maize price decreases. This result suggests, for example, that cash transfer programs could do more to boost nutrient consumption than maize input subsidies. Ellis and Maliro (2013) compare and contrast fertilizer subsidies and cash transfers by considering their roles in Malawi in recent years; they argue that the programs can serve complementary purposes and target different groups of beneficiaries. Fertilizer subsidies can be most effective when provided to farmers with the necessary resources to make productive use of them, and cash transfers are most necessary and appropriate for groups that are extremely resource-poor.
Existing Policies and Government Measures Affecting Food Security and Nutrition
The Government of Malawi has expressed its commitment to improving food and nutrition security in a variety of policies and institutional arrangements. It ranks second-best out of 45 African countries on the Hunger and Nutrition Commitment Index (HANCI), which evaluates countries based on their political commitment to tackling hunger and undernutrition (IDS 2017).
-
Malawi’s constitution includes the right to adequate nutrition, stating, “The State shall actively promote the welfare and development of the people of Malawi by progressively adopting and implementing policies and legislation aimed at achieving the following goals… Nutrition: To achieve adequate nutrition for all in order to promote good health and self-sufficiency” (WIPO 1998, 3).
-
The country’s third national development strategy, the Malawi Growth and Development Strategy (MGDS) (2017–2022), includes improved nutrition as a stated goal, describes the causes and implications of undernutrition in Malawi, and delineates the necessary strategies to overcome undernutrition (GoM 2017).
-
The National Multi-Sector Nutrition Policy (NMNP) (2018–2022), to be operationalized through the National Nutrition Strategic Plan (2018–2022), is a revision of the National Nutrition Policy and Strategic Plan 2007–2012. The Department of Nutrition, HIV and AIDS is the lead department responsible for the policy, but the roles of many other governmental and nongovernmental institutions are enumerated in the policy (GoM 2018b).
-
The goal of Malawi’s National Agriculture Policy, adopted in late 2016, is the following: “To achieve sustainable agricultural transformation that will result in significant growth of the agricultural sector, expanding incomes for farm households, improved food and nutrition security for all Malawians, and increased agricultural exports” (GoM 2016, 10). The policy explicitly acknowledges that Malawi has “over-concentrated” on maize and tobacco production in the past (GoM 2016, xi).
-
The National Agricultural Investment Plan (2017/18–2022/23) is the implementation and investment framework for the National Agriculture Policy (Mpaso 2018). It includes a detailed budget for each of 16 intervention areas, including food and nutrition security (GoM 2018a).
-
Other policies with the potential to provide support to the country’s nutrition objectives are the National Health Policy, the National Education Policy, the National Gender Policy, the National Resilience Strategy, the National Irrigation Policy, the Malawi National Social Support Programme II, and the Decentralization Policy (GoM 2018b; Chauwa 2018).
-
Malawi has been a member of the Scaling Up Nutrition (SUN) movement since 2011. The SUN network has recognized the country as an “early riser” because of its high level of political commitment to nutrition (Babu et al. 2016).
Policy and Institutional Recommendations for Moving Forward
While the Government of Malawi has expressed a strong commitment to food and nutrition security and has taken important steps to that end, more must be done to ensure effective multisectoral coordination and prioritization of resources to meet the challenges at hand (Compact2025 2016; Aberman 2019).
-
A draft Food and Nutrition Bill has been developed, which would legally establish for every person the right to adequate food and nutrition in national law. The bill has been developed in consultation with civil society organizations and other stakeholders (MMP 2017). Passage of this legislation by the Malawian parliament would be a positive step (SUN 2018).
-
The Department of Nutrition, HIV and AIDS is now part of the Ministry of Health rather than the Office of the President and the Cabinet. Given this transition, it is essential to ensure that nutrition continues to enjoy strong political support and efficient coordination between sectors (Babu et al. 2016).
-
As Malawi’s National Agriculture Policy acknowledges, the agricultural sector has an important role to play in achieving nutrition security in Malawi (GoM 2016). However, institutional arrangements and investment levels have not yet shifted to reflect this commitment to nutrition-sensitive agriculture. Incentives must be developed to ensure that the Ministry of Agriculture, Irrigation and Water Development prioritizes nutrition, such as by including a range of diet quality and nutrition indicators to measure the ministry’s progress on food security as a complement to maize production indicators, which are currently the primary measures of food security in Malawi (Aberman 2019).
-
Enabling low-income farmers to pursue agricultural diversification will require not only public support to ease household resource constraints, but also public-private partnerships to strengthen input and output markets. Current evidence shows that maize- legume intercropping has agronomic benefits, increases productivity, and reduces crop income variability (FAO 2019). Strategies to encourage increased intercropping, including maize-legume intercropping, should be pursued by the government, donors, and research institutions. Also, nutrition education should accompany interventions aimed at increasing agricultural diversification to help beneficiaries increase their dietary diversity.
-
Given the lifelong consequences of childhood undernutrition, evidence-based strategies for improving infant and young child feeding practices and improving child nutrition must be prioritized in order to maintain progress in this area. Considering the recent decline in breastfeeding rates and the valuable role of breastfeeding in child nutrition and survival, the government should ensure that adequate policies and resources are in place for the promotion of breastfeeding. Important steps include raising awareness about the importance of breastfeeding, providing support to working mothers who breastfeed, and continuously monitoring and enforcing the International Code on the Marketing of Breastmilk Substitutes.
-
The National Multi-Sectoral Nutrition Policy acknowledges the following challenges in terms of the enabling environment for nutrition: insufficient capacity (human and financial), unavailability of legal provisions to ensure nutrition security, and weak coordination and governance of structures at all levels (GoM 2018b). The government and supporting institutions must pursue strategies and resources to address these challenges.
-
Despite passage of the National Gender Policy in 2011, women and girls face persistent disadvantages in Malawi, including in terms of food and nutrition security, agriculture, education, health, and safety. Implementation of the National Gender Policy should be a priority for the government, the donor community, and NGOs alike to ensure that real progress can be made in the lives of women and girls (Compact2025 2016; Asfaw and Maggio 2018).
Footnotes
- The poverty rates expressed here are poverty headcount ratios at $1.90 per day (2011 purchasing power parity).
- This is in part because growth in agriculture generates higher returns for the factors of production held by poor people compared with growth in non-agricultural sectors and because growth in agriculture lowers the price of food, which occupies a high proportion of the budget of poor households (Dorosh and Thurlow 2018).
- Globally, undernutrition is responsible for 45 percent of deaths among children under age five (Black et al. 2013). For a detailed explanation of child mortality’s inclusion in the GHI, see Wiesmann et al. 2015.
- Poor fetal growth or stunting in the first two years of life is associated with delayed child development, reduced earnings in adulthood, and chronic diseases, and maternal short stature results in difficult births and poor birth outcomes (Leroy and Frongillo 2019).
- Concern Worldwide, a partner in the Global Hunger Index, was instrumental in developing the community-based management of acute malnutrition (CMAM) program in Malawi (Kathumba 2012).
- A “minimum acceptable diet” is a standard that combines minimum dietary diversity and minimum meal frequency, with different recommendations for breastfed and non-breastfed children, who need to receive milk or milk products as a substitute for breast milk. This measure was not included in Demographic and Health Survey (DHS) reports before 2010 so earlier comparisons are not possible.
Authors
Jill Bernstein and Doris Wiesmann