Malawi:
Building Resilient Systems for Food and Nutrition
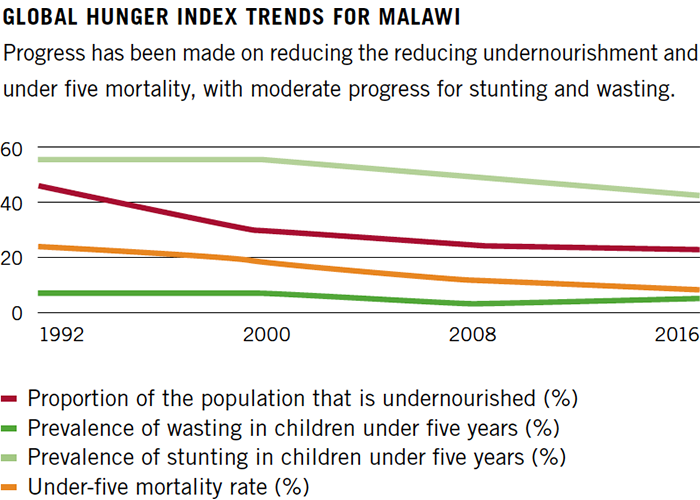
A landlocked country with an estimated population of 17.2 million, Malawi has experienced rapid recent growth in the agricultural sector. The proportion of malnourished children remains one of the highest in the world. With a 2016 GHI score of 26.9, Malawi’s hunger score is categorised as serious.
20.7%
of the population is under-nourished, meaning they do not receive enough calories per day
37%*
of children under five are stunted (low height for their age), reflecting chronic undernutrition
* preliminary data from DHS Survey Malawi 2015/16
Farming is the mainstay of Malawian life. More than 80% of the population is reliant on subsistence farming, with the main staple being maize.
Macroeconomic instability coupled with the impact of climate change and El Niño in particular have hit the country hard in recent years, with floods and droughts causing devastation for many of Malawi’s smallholder farmers and increasing the rate of acute malnutrition across the wider population. While crop diversification is an explicit goal of the Government of Malawi, the steps towards this goal and the pathways towards improved nutritional outcomes are challenging, as highlighted by the International Food Policy Research Institute (IFPRI, 2015).
A high population growth rate and fertility rate (3.07%, and an ‘average total fertility rate’ of 4.4 in 2014 according to the World Bank) among young women further compound the challenge to ensure food security and the provision of adequate basic services to vulnerable Malawians.
The 2016 Global Hunger Index reports that the hunger situation in Malawi as ‘serious’. According to the Malawi SMART Survey 2016, one in three households are classified as experiencing inadequate food consumption, while the conclusion of the Malawi Vulnerability Assessment Committee (MVAC) in its annual assessment and analysis is that 6.5 million people – or 1 in 3 Malawians – will be unable to meet their minimum food requirements in 2016/2017.
The issue of chronic malnutrition is also one of grave concern. According to the preliminary report recently published by the Demographic Health Survey (DHS), 37% of children under the age of five are considered short for their age or stunted, with 11% being severely stunted. While this figure has fallen compared to 42% in 2014 and 47% in 2010, the figures are nevertheless alarming.
Concern Worldwide has been working in Malawi since 2002, supporting the Government in its efforts to tackle malnutrition and working with communities on a range of interventions, from emergency response to livelihoods, healthcare, nutrition, and education. Throughout the course of 2015, Concern Malawi reached over 380,000 people directly. As well as helping farmers improve production, the focus is increasingly on encouraging consumption by educating farmers about nutrition.
As one of the first countries to pilot and adopt a community-based management approach to malnutrition – as well as one of the first to become a member of the Scaling Up Nutrition (SUN) movement – Malawi has demonstrated its political commitment to addressing undernutrition. Furthermore, at the Nutrition for Growth event hosted in the UK in 2013, Malawi made several financial and policy-related commitments, which have survived several changes in Government, thereby illustrating broad policy-based support.
Resource allocation, however, remains low. The causes of malnutrition in Malawi are numerous and multifaceted, from direct factors to underlying contributors. Reaching ‘zero hunger’ will require a comprehensive approach across sectors and stakeholders that focuses on the range of causes. The effective scaling up of prevention and treatment interventions are essential to this work. This study looks back at a specific initiative around the treatment of malnutrition, which Concern and the Malawian Government partnered on and invested significantly in, and from which much learning can be drawn.
It reflects on the gains made and the challenges faced, before looking to the future and the evolving focus on prevention of undernutrition through programmes, partnerships, advocacy and improved maternal and child health services. The study is supported by desk research and a range of interviews carried out in July 2016 at national level and within the district of Mchinji.
It is inspired by Concern Malawi’s stated goal that ‘extremely poor households have improved food and nutrition security and increased resilience to shock and hazards’ (Strategic Plan 2014-2018).
Institutionalising Community-based Management of Acute Malnutrition: Experience and Learning to Date

I enjoy the chance to teach mothers in the community. I’ve learnt about good sanitation, hygiene and nutrition. I know the importance of the six food groups now and I’ve been able to pass this onto other mothers. Josephine Oscar, Lead Mother in SNIC project, Zizwa Village, Mchinji

Before, the children were eating a corn-only mix. We received the seeds and training to harvest more crops and now they have a more diverse diet. Lustilla Mathew, Caregiver in CBCC, Mbachundu village, Mchinji
3%*
of children under five are wasted (low weight for their height), reflecting acute undernutrition
6.4%
of children die before the age of five
* preliminary data from DHS Survey Malawi 2015/16
Between 2002 and 2006, Concern Worldwide partnered with Valid International to pilot a community-based approach to addressing acute malnutrition in Malawi. The approach has four key components:
-
COMMUNITY MOBILISATION: outreach to raise awareness, screening and identification of cases in the community using a middle-upper arm circumference band (MUAC), and follow-up with caregivers and malnourished children.
-
SUPPLEMENTARY FEEDING PROGRAMS: provision of takehome rations (e.g. fortified blended foods) and routine medical care for children with moderate acute malnutrition.
-
OUTPATIENT THERAPEUTIC PROGRAM: provision of high-energy therapeutic food and regular check-ups for children who are severely malnourished without medical complications. As a key point, the children are treated at home in their communities.
-
NUTRITION REHABILITATION UNITS: provision of inpatient care for acutely malnourished children with medical complications.
By 2004, the Malawi pilot project had demonstrated excellent treatment outcomes, achieved high coverage, received a high level of acceptance from the community and proved to be a cost-effective solution to expensive inpatient treatment.
In 2006, the Ministry of Health announced its intention to standardise this approach, which became known as Community-based Management of Acute Malnutrition (CMAM), and to scale it up to incorporate all 29 districts across the country. A five-year partnership between Concern Malawi and the Government was established to develop the capacity of the CMAM delivery services at all levels, including the rollout of guidelines and policy and the standardisation of service provision.
Another aim of the partnership was to advocate the scaling up and integration of the approach into the health system. To facilitate this work, the CMAM Advisory Service (CAS) was established, with funding support from USAID. In 2013, the Ministry of Health assumed all of the key functions as Concern took a step back from the project.
By this time, CMAM services were available in all districts. The approach had been integrated into national policies and guidelines and into the existing health infrastructure in terms of training, supply management and supervision. Focal points were identified at all levels, national and district-level training teams were established, supervision was incorporated into District Health Offices, and evidence and learning was documented. District Health Officers were trained on how to budget for CMAM and instructed on how to factor costs into district implementation plans.
A considerable amount had been achieved. Alongside these successes and achievements, however, issues arose once external support ceased with regard to the sustainability of the approach and the comparative inability to adapt CMAM for government-level systems.
The final evaluation of the Community-based Therapeutic Care Institutionalisation in Malawi carried out towards the end of 2013, at the request of USAID and the Canadian International Development Agency, highlighted a number of challenges:
- while CAS had helped to extend capacity and scale up CMAM services at national level, those services had not been fully institutionalised/integrated into the health system
- organisational development within the Ministry of Health that would enable it to assume the project’s advisory and technical functions at sub-national level had not been part of the project design and did not take place
- there was a lack of alignment of CAS activities in conjunction with the decentralisation process
To assess the effectiveness of CMAM coverage, the government subsequently carried out a bottleneck analysis in 2014, which highlighted some further challenges, including:
- inadequate supply of CMAM commodities
- a lack of adequately trained staff to implement CMAM, with few clinicians, nurses and health surveillance assistants having received comprehensive CMAM training
- low levels of effective coverage, with 36% of severe acute malnutrition and 15% of MAM cases discharged as cured, thus demonstrating the poor quality of case management
The interviews conducted for this study supported many of these findings and raised further issues for reflection, including the challenge of securing funding to support health services and thereby overcome these institutional issues. Other challenges which persist are highly practical in nature. Many Health Surveillance Assistants (HSAs) and other health staff are overstretched and under-motivated. Supply management and the timely delivery of supplies are sometimes problematic, and ‘readyto-use therapeutic foods’ are unavailable at times. There is also a heavy reliance on support from external agencies and organisations to acquire the necessary supplies.
A lack of transport and fuel is also cited as a practical problem facing health staff at district level. HSAs are responsible for carrying out growth monitoring in villages on a monthly basis and, along with District Nutrition Officers, are meant to make regular visits to communities in order to monitor CMAM activities. A lack of transport impedes their ability to carry out active case findings and screenings and to make referrals.
The acquisition of data and how it is used for decision-making is another challenge. CMAM data passes through a number of steps and channels, and delayed submissions can affect the timeliness of a response. District Nutrition Coordination Committees (DNCC), which bring together key nutrition stakeholders, are supposed to receive and discuss consolidated health facility information. However, this does not always happen due to time constraints and an irregular meeting schedule.
In addition, the monitoring and admission forms which health staff are expected to complete are complex, with some staff feeling unable to complete certain sections. Further, while each HSA has the support of around 10 health volunteers in the community, training for volunteers tends to vary, with different training being provided to different volunteers depending on the donor and project being implemented. Out of a team of ten, only three volunteers may be trained in CMAM. No standard training ‘package’ is provided.
Addressing the Challenges: National Nutrition Policy 2016-2020
{kind=link}
The Government has recognised these challenges and the need to address them, and has been working on a new 2016-2020 National Nutrition Policy.
It has also prepared an accompanying Operational Plan, which explicitly recognises the barriers to institutionalisation and effective coverage of CMAM delivery, seeking to deal with them in a comprehensive manner.
The policy highlights the low capacity and participation of clinicians in the management of severe acute malnutrition, insufficient community outreach and mobilisation, weak supply chain management and the overall low quality of CMAM service delivery. Some of the strategic areas for action include:
- enhancing the institutional and human capacity of service providers
- improving availability and access to CMAM supplies and equipment
- increasing government ownership and financing of acute malnutrition interventions
- pre-service and in-service training which will be prioritised under the new policy
The operational plan also seeks to improve the current institutional arrangement for coordinating CMAM at national, district, health facility and community levels, as well as strengthening the links between CMAM and other nutrition-specific and nutrition-sensitive interventions. Attention will also be given to the generation and use of accurate and reliable monitoring and evaluation data.
This new policy and plan is arriving at a time when action and ambition are essential, especially given seasonal climate change-related shocks. Although spikes in cases of acute malnutrition may be becoming increasingly predictable, there is no system in place at district level to plan for, identify or provide a rapid response via a ‘surge mechanism’, instead relying on short-term emergency responses by government and partners.
From CMAM to CMAM Surge
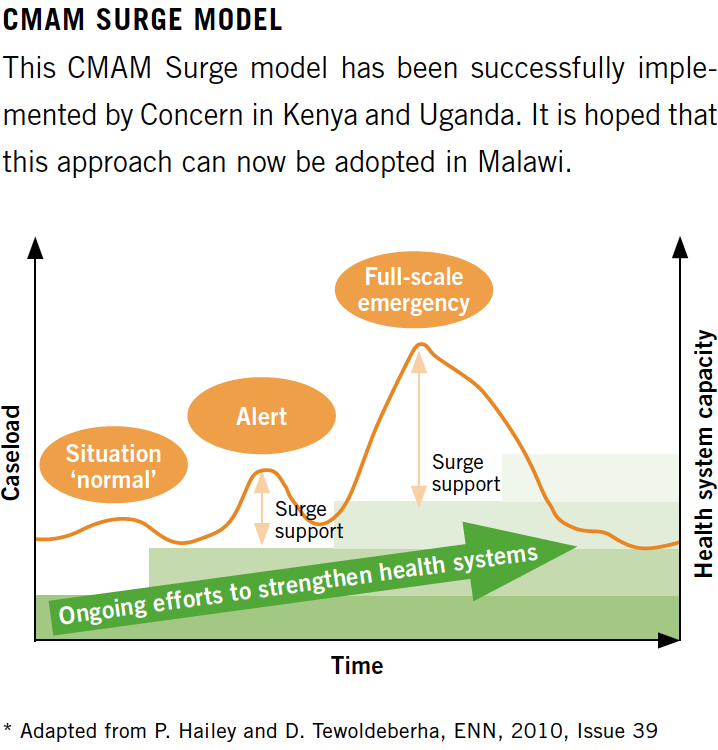
To address this challenge and to play a further role in supporting the Government’s efforts, Concern Malawi is designing a CMAM Surge capacity-building programme that comprises a set of tools intended to assist government health teams to respond to surges in acute malnutrition more effectively while building health system resilience over the long term.
An emergency nutrition response often runs parallel to the health system and is implemented in ‘startstop’ episodes of external response. The Surge programme aims to (i) strengthen the capacity of the health structures at district level and (ii) encourage coordination bodies to use early warning information for decision-making and response. Interventions focus on two core areas: health facility-level surveillance and district coordination capacity.
Health facility staff are encouraged to analyse and contextualise the drivers of seasonal spikes and increased caseloads of acute malnutrition. They identify the thresholds that are intended to trigger additional support and monitor against these thresholds on a monthly basis. The thresholds are set by each health facility. Once exceeded, the health facility notifies the district, mobilises its own resources, and, if necessary, requests the provision of additional support, thereby enabling the facility to cope with an increased caseload without compromising the quality of the health services. The provision of surge support, including the type and level of support and how and when to scale up and down, is agreed at district level prior to implementation of the approach.
From Treatment to Prevention:
Reaching Zero Hunger Faster
61%
of children are exclusively breastfed for 6 months
Source: Malawi DHS 2015-2016
57/60
Life expectancy (m/f)
Source: World Health Organisation, Latest data available from the Global Health Observatory

Before we started teaching the programme, only a few houses in my village had toilets. Many more households have built them now after learning about the benefits. Also, more women understand the importance of antenatal visits and go to the doctor when pregnant. I became a Care Group Promoter because I wanted to help my people to live healthier lives. Gift Kamanga, Farmer and volunteer, Care Group Promoter, Mkanda village, Mchinji
Concern is also committed to looking beyond the treatment of undernutrition.
It is placing an increased focus on prevention and working with the Government to this end. The Government of Malawi is well aware of the need for a comprehensive, sustainable approach to undernutrition, and has therefore declared its support for the recently launched Sustainable Development Goals (SDGs). The Government has included the prevention and treatment of malnourished children in its critical national development priorities as part of the Malawi Growth and Development Strategy II (2011-2016). The management of acute malnutrition is also a key goal of the Malawi Health Sector Strategic Plan (2011-2016), the National Nutrition Policy 2016-2020, and the Infant and Young Child Feeding Policy 2009.
Furthermore, the prevention of undernutrition is the first priority area under the revised National Nutrition Policy. The policy aims to build on lessons learned and achievements made over the past decade, and will promote the implementation and integration of high-impact, nutrition-specific and nutrition-sensitive interventions across the relevant core sector policies, strategies, implementation plans and budgets.
The government has been partnering with the World Bank and the Canadian International Development Agency (CIDA), which have supported the Nutrition and HIV/AIDS project since 2012. One aspect of this project is the ‘Support for Nutrition Improvement Component’ (SNIC), which is being implemented in 15 districts across the country with support from a range of implementing partners. The project aims to strengthen service delivery by increasing access to and utilisation of services which are known to contribute to a reduction in child stunting and maternal and child anaemia. In March 2014, Concern began its support of SNIC, becoming the implementing partner in the district of Mchinji, which, according to the 2010 DHS, has the fourth-highest stunting rate in the country at 54%. Through its support of SNIC, Concern has adopted a multi-sector approach that links nutrition education, social and behavioural change, water and sanitation, food security and local capacity building.
Community mobilisation is a core strategy for ensuring that nutrition-based interventions are sustainable, benefit from ownership at local level and increase participation in and knowledge and adoption of optimal practices. Concern supports the establishment of community structures and groups and their capacity-building processes.
The founding of Care Groups – consisting of around a dozen Lead Mothers – is a key way to improve access to a minimum package of care and services for mothers in the community. Care Group Promoters support these Care Groups and facilitate group sessions, individual counselling and home visits. Promoters receive training on sanitation and hygiene, maternal nutrition, exclusive breastfeeding and complementary feeding. This training is passed on to Lead Mothers, who in turn support other mothers in the community.
While they are eager to help their communities, the retention and motivation of Promoters and Care Group Lead Mothers can be challenging, as there is an expectation of financial incentives. When asked about additional training that they wish to receive, Promoters suggested training on how to deal with gender-based violence and malaria. They also pointed out how overstretched they can be and were conscious of the fact that the support they provide is not always enough, with one Promoter estimating that he was only able to access 80% of the community.
Care Groups, meanwhile, face their own challenges. At first, the mothers these groups worked with, in the community, were reluctant to adopt the measures promoted through the training. A common barrier identified by the Lead Mothers was the lack of available diversified foods and seeds, making it difficult for cluster members to apply the lessons they had learned about diversifying one’s diet. To address this and to provide a more comprehensive approach, Care Groups are now provided with vegetable seeds, including orange-fleshed sweet potato vines, groundnuts and fruit trees saplings, and the mothers become members of a goat-sharing pass on scheme.
As part of a continuum of care, additional key objectives of the programme are to ensure that children who suffer from wasting are identified and are able to be referred for treatment. Health volunteers and Village Development Committees (VDCs) receive training on active case finding.
Furthermore, support is given to Community-based Child Care Centres (CBCC), which facilitate early child development for children under the age of five. CBCCs have proved to be a key entry point with regard to increasing coverage of health and nutrition interventions and connecting children with health services. Concern has been providing inputs for vegetable gardens as a means of enabling CBCC caregivers to provide more nutritious food for the children. Support also includes the provision of water filters, hygiene promotion training and growth monitoring training. Many other interventions implemented by NGOs partnering with the Government (e.g. Alliance 2015 member Welthungerhilfe’s school feeding programme and Alliance2015 projects by other organisations involving care groups) have shown good results and generated strong learning and scaling-up potential.
The Way Forward

I’ve seen a change in how the cluster members and the Lead Mothers practice hygiene and sanitation. I feel good to be encouraging women to change their behaviour for the better and to be helping my community. Ireen Chinglanda, Volunteer Care Group Promoter, Mkanda village, Mchinji
8%
of children age 6-23 months are fed in accordance with a minimum acceptable diet
Source: Malawi DHS 2015-2016
Over the last decade, Malawi has shown leadership in the area of nutrition through its innovative nutrition journey. The revised National Nutrition Policy and Operational Plan provide strong guidance and direction on a way forward.
According to a budget analysis carried out by the Civil Society Organisations Nutrition Alliance (CSONA) and Save the Children for the 2016/2017 budget, the government of Malawi has reached its N4G commitment to spend 0.3% of its overall budget on nutrition. This is to be commended. There is a real need, however, for additional domestic resources. With an estimated 1.268 million stunted children in Malawi (CoHA 2015), the government spends an average of MWK 268 (USD 0.35) per child on nutrition interventions.
Moreover, there remains a heavy reliance on support from external agencies and organisations when it comes to implementing CMAM programming and carrying out active case finding.
The government of Malawi is committed to improving the quality of its nutrition programmes. Lessons learned so far highlight the importance of ensuring that there are formal structures and operating procedures in place. Given the context of cyclical crises, there is a clear need to work with and strengthen the health system. Revised CMAM guidelines are in the process of being finalised and a series of training courses are planned as part of its rollout. This will provide the opportunity to include and plan for the dedicated mentoring of health staff. With the increased emphasis on ensuring a continuum of care in mind, the Government is working to strengthen its links between sector-based and stakeholder programmes at district level.
To support this, joint plans and the coordination of interventions at facility level are pivotal if the overall impact and quality are to be improved. By way of example, clear links between CMAM programmes and care groups need to be established. Imperative to this will be connecting children who have been discharged from a CMAM programme with a care group in their community. To support this, the integration of mass routine screening into the regular day-to-day responsibilities of the HSAs needs to be defined more clearly.
Utilisation of the existing system can be improved, making use of child health days and other opportunities and channels such as CBCCs to support screenings and the promotion of nutrition-based communication and support.
Malawi is in the process of finalising its National Development Plan. This provides the opportunity to build on the lessons learned and experience gained to date and to sustainably embed Malawi’s commitment to addressing malnutrition, thereby ensuring that nutrition remains a priority in terms of policy and programmes. The new plan will see Malawi consolidating its development efforts in order to achieve the SDGs.
The foundations are in place. With sustained prioritisation and increased resource allocation from domestic and international sources, Malawi can make great strides towards ensuring that zero hunger and the sustainable development goals are achieved.